Remote Anchorage Solutions for Atrophic Maxilla: Application of the PATZi Protocol in Patients at the
Faculty of Dentistry, UFM – A Case Series
Jimmy Sandoval 1)Rodrigo Cayarga 1,3)Erick Lima 1,3)Luis Grisolía 2,3)Juan Gonzalez 3)
1) Advanced Implantology Department. Faculty of Dentistry, Francisco Marroquín University, Guatemala.
2) Restorative Department. Faculty of Dentistry, Francisco Marroquín University, Guatemala.
3) Continues Education Department. Faculty of Dentistry, Francisco Marroquín University, Guatemala.
Abstract
Maxillary bone atrophy, characterized by reduced bone density and diminished height and thickness, presents significant challenges during the surgical and restorative phases of dental implant treatment. Traditional rehabilitation with mucosa-supported complete dentures often leads to patient discomfort, limited prosthetic stability, and progressive alveolar bone resorption. In contrast, implant-supported prostheses have emerged as a superior solution, offering improved retention, stability, and masticatory function. However, bone volume deficiency and inadequate anterior-posterior spread often complicate implant placement in atrophic maxillas.
The PATZi protocol has been developed as a systematic approach to addressing these challenges, utilizing both conventional and remote anchorage dental implants to optimize prosthetic rehabilitation in atrophic maxillas. This protocol enables the immediate loading of provisional fixed prostheses through a structured algorithm that prioritizes implant placement based on anatomical suitability and primary stability.
The sequence begins with pterygoid implants (P1) and proceeds to anterior bicortical anchorage sites (A1 or A2), followed by conventional angled implants in the premolar region (T1 or T2). Zygomatic implants (Z1, Z2, Z3) serve as a last resort in cases of insufficient stability.
By establishing a clear surgical framework, the PATZi protocol ensures consistent outcomes and facilitates immediate prosthetic loading, with a recommended insertion torque of at least 30 Ncm per implant or a total of 120 Ncm. This innovative approach enhances patient satisfaction, prosthetic function, and long-term success in the rehabilitation of atrophic maxillas.
Maxillary bone atrophy is defined as bone resorption that is clinically observed as a decrease in bone density and a reduction in height and thickness, complicating both the surgical and restorative phases of dental implant treatment.1 The rehabilitation of these patients is challenging, as achieving prosthetic stability, proper phonetics, and stable masticatory function remains a major concern.2
Traditionally, treatment for these patients has relied on mucosa-supported complete dentures—acrylic devices designed to replace lost and/or atrophied soft and hard tissues. These removable prostheses are strictly supported by the maxillary mucosa.1 However, complete dentures have notable disadvantages, including poor stability, inadequate support and retention, and patient discomfort, as they can cause soft tissue irritation.3 Furthermore, their use can contribute to continuous alveolar bone atrophy, affecting both vertical and horizontal bone dimensions.2
The ideal solution for these patients is an implant-supported prosthesis, which offers superior retention, stability, and masticatory function, ultimately improving patient quality of life.4 The All-on-4 configuration, introduced by P. Maló,5 has been widely adopted for implant-supported prosthetic rehabilitation. However, one of the primary challenges in implantology remains insufficient bone volume and inadequate anterior-posterior spread.6
In this context, the PATZi protocol has emerged as a promising technique for prosthetic rehabilitation in atrophic maxillas. This systematic algorithm integrates conventional dental implants (angled, parallel) and remote anchorage dental implants (pterygoid, nasopalatine, nasal spine, transnasal, transsinusal, zygomatic) in a logical sequence, with the primary goal of enabling immediate loading of a provisional fixed prosthesis.6
The PATZi protocol provides a structured surgical sequence for implant placement in atrophic maxillas. It begins with the placement of pterygoid implants (P1) in the molar region of the maxilla. If adequate primary stability is not achieved, the implant is classified as failed (Px).6,7
The next step involves placing implants in the anterior region of the maxilla with bicortical anchorage. Anatomical sites such as the nasal spine, piriform bone, and lateral nasal wall are used (category A1). If these areas are contraindicated, transnasal implants are placed (category A2). If the required insertion torque is not achieved, the implant is classified as failed (Ax).6,7
Conventional angled implants are then placed in the premolar region without bicortical anchorage (category T1). If this is not feasible, remote anchorage in the lateral nasal wall is used (category T2). If primary stability is not obtained, the implant is classified as failed (Tx).6,7
Finally, if any of the previous categories fail, zygomatic implants serve as a last resort. These can be placed in the premolar (Z1), molar (Z2), or anterior (Z3) region, depending on the implant emergence site.6,7
The PATZi protocol provides a systematic and structured framework for placing dental implants in atrophic maxillas, ensuring an optimal biomechanical configuration and facilitating the immediate loading of implant-supported prostheses. While no specific minimum insertion torque has been established, a minimum of 30 Ncm per implant or a total insertion torque of 120 Ncm is generally required for immediate loading.6
By following this protocol, surgeons can achieve consistent outcomes while effectively planning for any necessary future interventions.
The PATZi protocol applied:
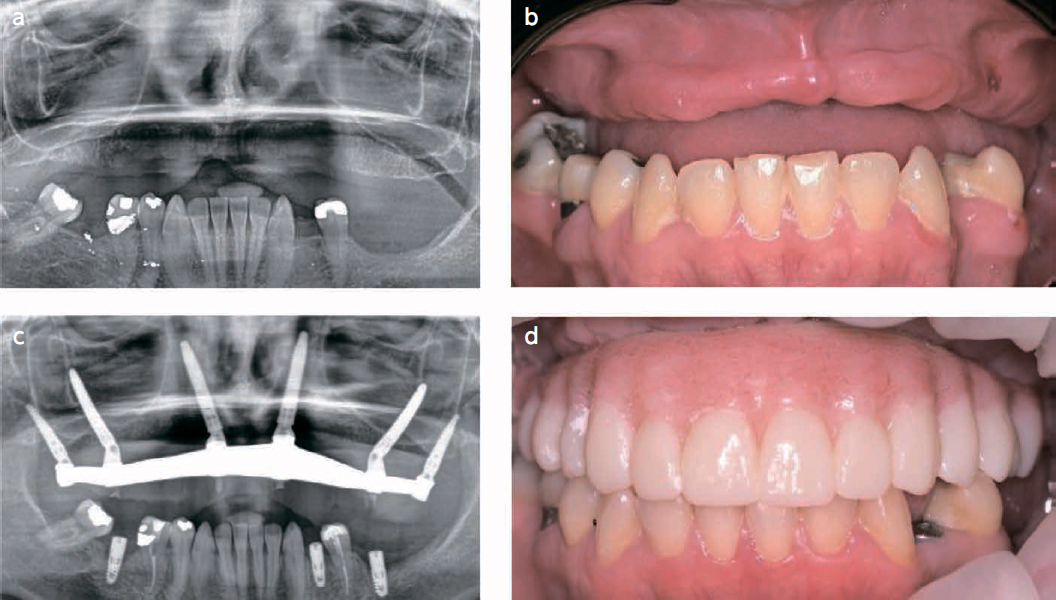
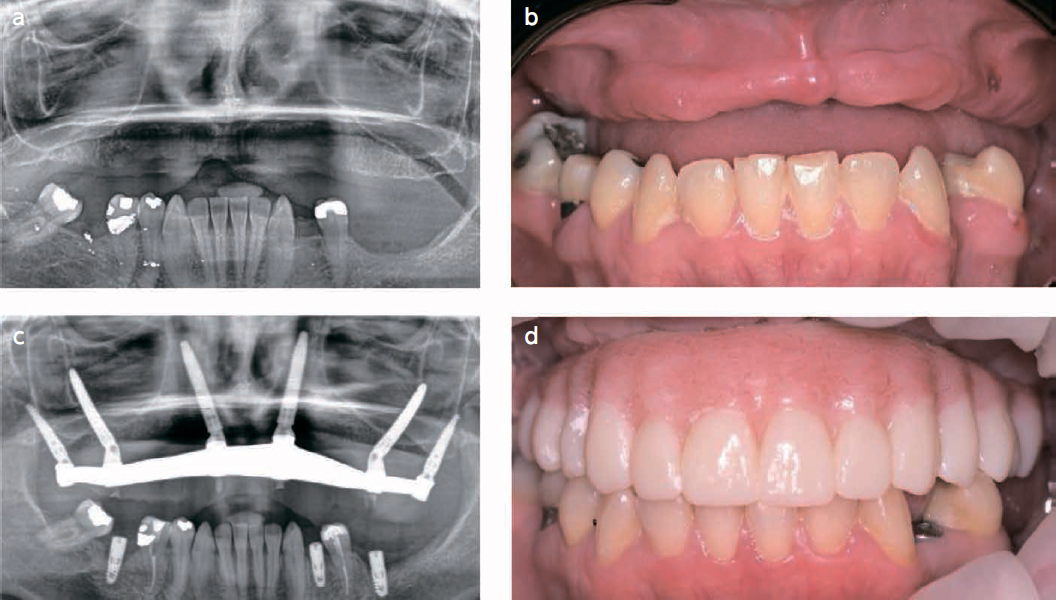
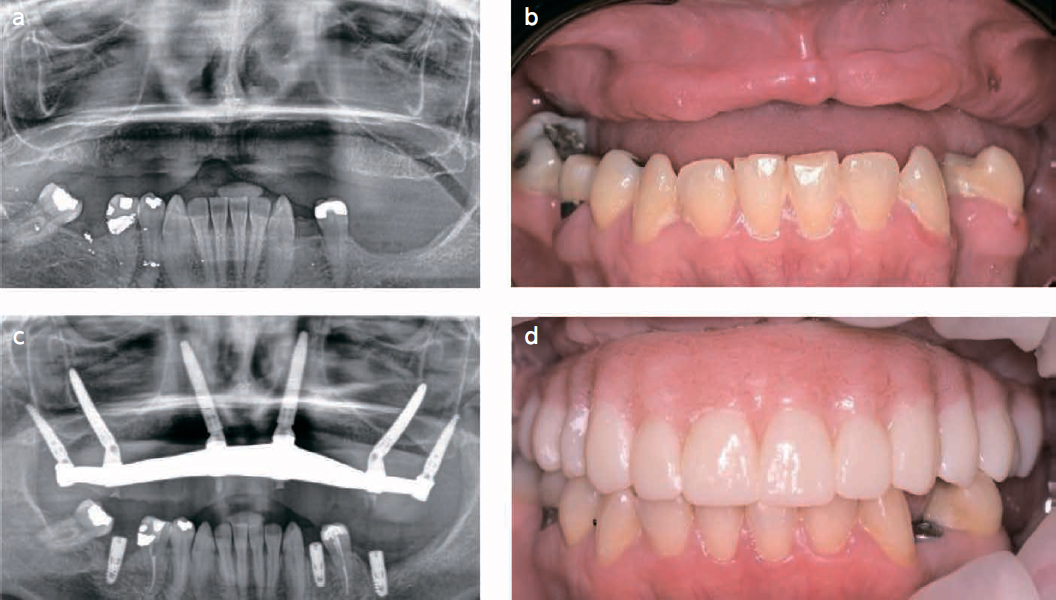
(Fig.1)
a) Female patient, 44 years old, with bone loss due to periodontal disease and a traumatic
injury.
b) Clinical situation of the patient, before the surgery.
c) Following the PATZi algorithm in this case, first pterygoid implants were placed bilaterally P1, attention was then directed to the anterior region, where bilateral intra alveolar implants don’t achieve a primary stability, so extra alveolar implants that engaged the lateral nasal wall bone were achieved A2, traditional tilted implants and transsinus implants were attempt and don’t show primary stability Tx. PATZi protocol demonstrates the indication for zygomatic implants, so Z1 configuration zygomatic implants were placed satisfactorily.
d) Clinical photography, after delivery of the final prothesis, rehabilitation with hybrid prothesis after 6 months.
Objective:
The purpose of this case series is to contribute to documentation by presenting the application of the PATZi protocol in atrophic maxilla.
Materials and Methods
A total of 15 patients with atrophic maxillae were treated at the Faculty of Dentistry, Francisco Marroquín University between January 2023 and October 2023. Surgical procedures were performed using the PATZi protocol by the O.R.C.A.A. surgical team.
Implant Placement Summary
A total of 112 dental implants were placed, including:
30 pterygoid (P) implants
30 anterior (A) implants
30 tilted (T) implants
Due to insufficient primary stability (≥35N) for immediate prosthesis loading and to
enhance anteroposterior distribution, an additional 22 zygomatic implants (Zi) were placed as follows:
10 implants emerging in the premolar region (Z1)
8 implants emerging in the molar region (Z2)
4 implants emerging in the anterior region (Z3)
Data Collection & Evaluation
Preoperative demographic data were recorded.
Primary stability of immediate implants was assessed.
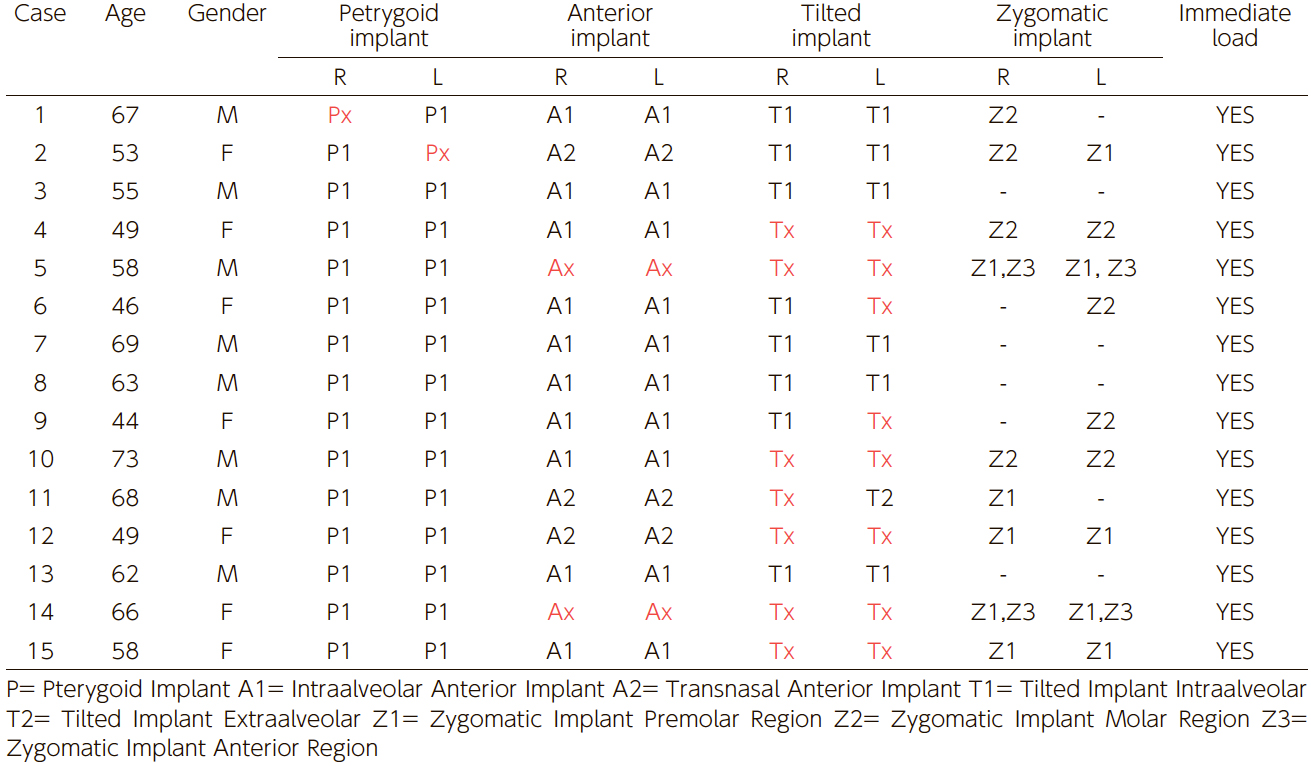
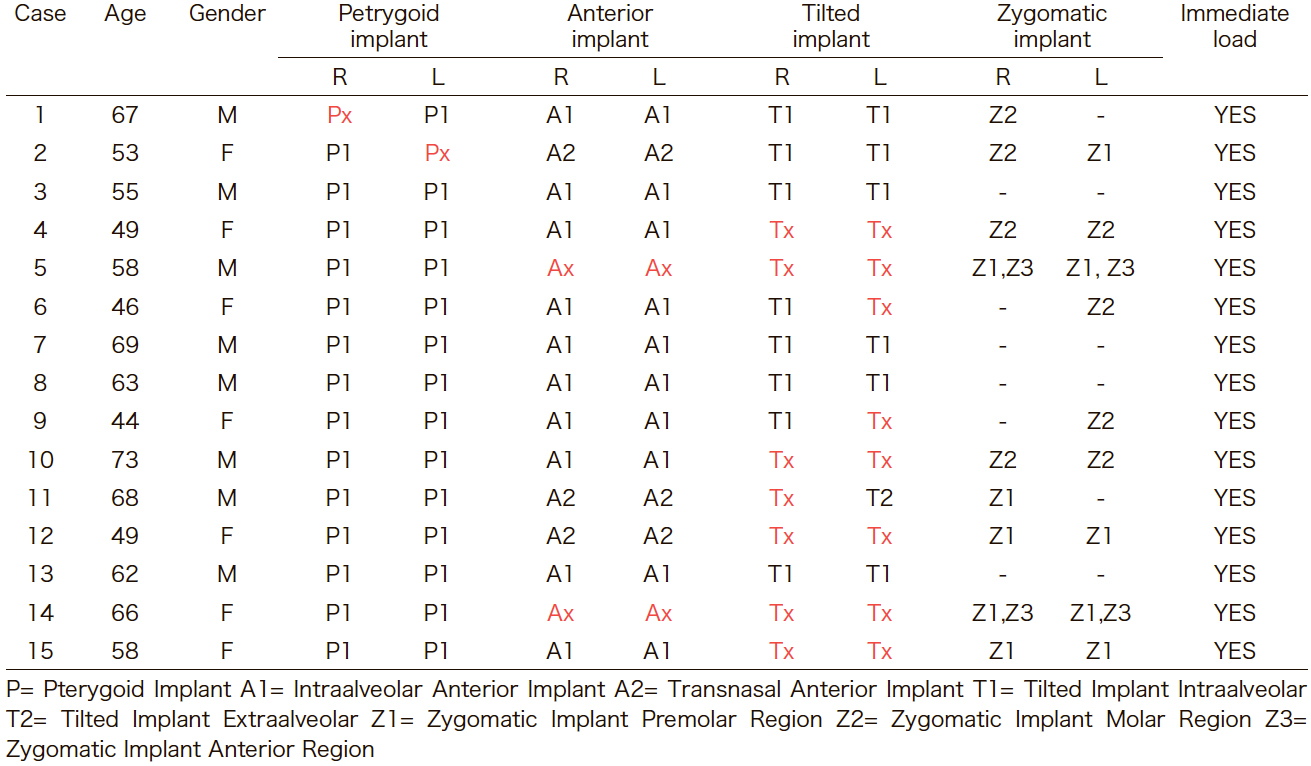
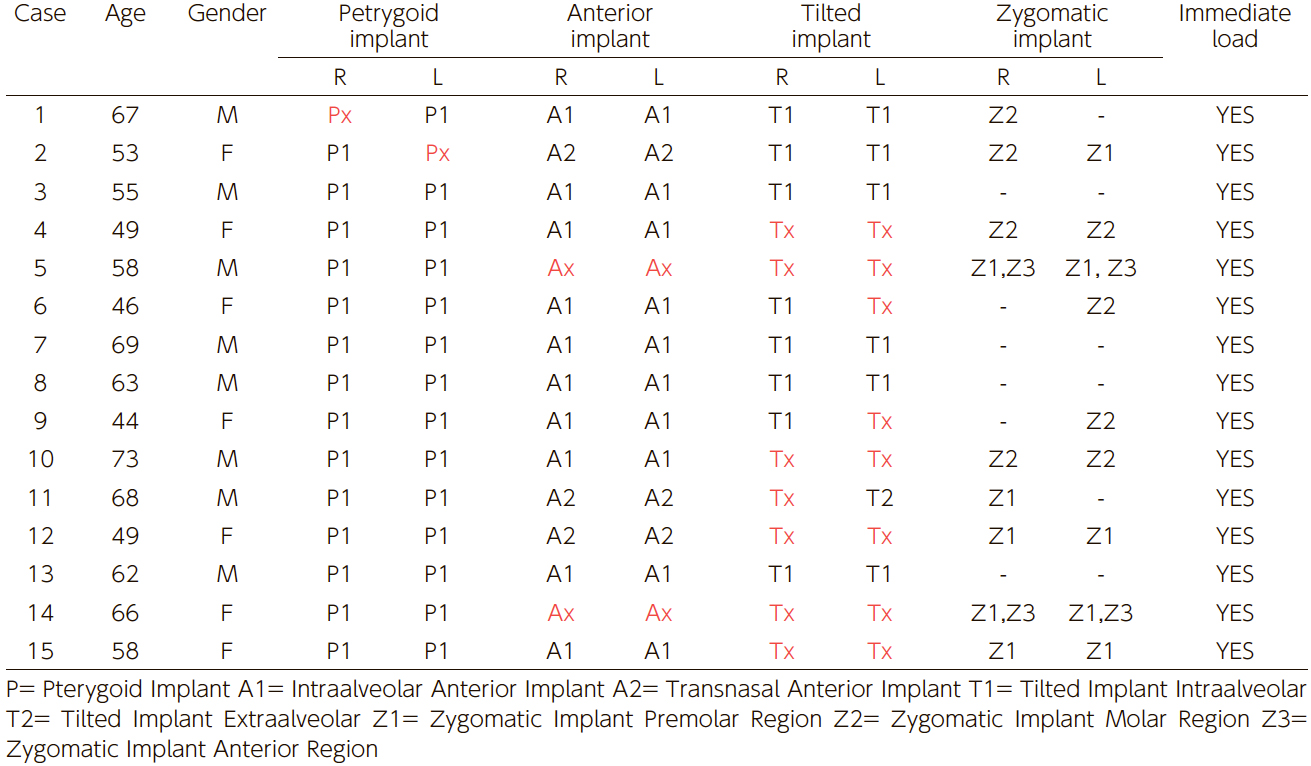
Immediate loading feasibility after surgery was evaluated (Table 1).
(Table 1) Demographics, primary stability of implant and prosthesis immediate load.
Results:
The 15 patients treated with the PATZi protocol, 7 were female and 8 were male, with an age range of 44 to 73 years. Of the 112 implants placed, 28/30 pterygoid implants, 26/30 anterior implants (20 intra-alveolar (A1), 6 transnasal (A2)), and 15/30 tilted implants showed primary stability. All patients received immediate loading of dental implants after the surgery.
Conclusions and clinical implications:
The PATZi protocol, in the hands of expert clinicians, incorporating both conventional and remote anchorage implants, resolves cases of severe maxillary atrophy and is a viable alternative to achieving primary stability and obtaining immediate loading of dental implants. In particular cases where primary stability for immediate loading and adequate anteroposterior distribution were not achieved, the placement of zygomatic implants is indicated.
However, the observation period in this study may be too short to assess the long-term success or failure of the protocol fully. Follow-up observations should include evaluating the longevity of the implants, assessing prosthetic stability, and monitoring potential complications such as implant failure, bone resorption, or prosthesis misfit. Regular post-surgical assessments, including radiographic analysis and clinical examinations at 6 months, 1 year, and annually thereafter, would provide a more comprehensive understanding of the protocol's long-term efficacy and safety. Future studies with longer follow-up periods are essential to validate these findings and further refine the application of the PATZi protocol.
References:
The Glossary of Prosthodontic Terms 2023: Tenth Edition. (2023). The Journal of prosthetic dentistry,
130(4 Suppl 1), e1–e3.
Bedrossian, E., Sullivan, R. M., Fortin, Y., Malo, P., & Indresano, T. (2008). Fixed-prosthetic implant restoration of the edentulous maxilla: a systematic pretreatment evaluation method. Journal of oral and maxillofacial surgery : official journal of the American Association of Oral and Maxillofacial Surgeons, 66(1), 112–122.
Zarb, George & Bolender, C.L.. (2004). Prosthodontic treatment for edentulous patients: complete dentures and implant-supported prostheses. 12 th ed. St. Louis: Mosby Inc. 190-207.
Schwarz F, Schär A, Nelson K, Fretwurst T, Flügge T., & Ramanauskaite A, Recommendations for Implant-Supported Full-Arch Rehabilitations in Edentulous Patients: The Oral Reconstruction Foundation Consensus Report. International Journal of Prosthodontics. 2021;34.
Maló, P., Rangert, B., & Nobre, M. (2003). "All-on-Four" immediate-function concept with Brånemark System implants for completely edentulous mandibles: a retrospective clinical study. Clinical implant dentistry and related research, 5 Suppl 1, 2–9.
Ponnusamy, S., Gonzalez, J., & Holtzclaw, D. (2023). A systematic approach to restoring full arch length with maxillary fixed implant reconstruction: The PATZi protocol. The International Journal of Oral & Maxillofacial Implants, 38(5), 996-1004.
Holtzclaw, D. (2023). Remote anchorage solutions for severe maxillary atrophy: Zygomatic implants, pterygoid implants, transnasal implants, piriform rim implants, nasopalatine implants, and trans-sinus dental implants. Zygoma Partners, LLLP
The Glossary of Prosthodontic Terms 2023: Tenth Edition. (2023). The Journal of prosthetic dentistry,
130(4 Suppl 1), e1–e3.
Bedrossian, E., Sullivan, R. M., Fortin, Y., Malo, P., & Indresano, T. (2008). Fixed-prosthetic implant restoration of the edentulous maxilla: a systematic pretreatment evaluation method. Journal of oral and maxillofacial surgery : official journal of the American Association of Oral and Maxillofacial Surgeons, 66(1), 112–122.
Zarb, George & Bolender, C.L.. (2004). Prosthodontic treatment for edentulous patients: complete dentures and implant-supported prostheses. 12 th ed. St. Louis: Mosby Inc. 190-207.
Schwarz F, Schär A, Nelson K, Fretwurst T, Flügge T., & Ramanauskaite A, Recommendations for Implant-Supported Full-Arch Rehabilitations in Edentulous Patients: The Oral Reconstruction Foundation Consensus Report. International Journal of Prosthodontics. 2021;34.
Maló, P., Rangert, B., & Nobre, M. (2003). "All-on-Four" immediate-function concept with Brånemark System implants for completely edentulous mandibles: a retrospective clinical study. Clinical implant dentistry and related research, 5 Suppl 1, 2–9.
Ponnusamy, S., Gonzalez, J., & Holtzclaw, D. (2023). A systematic approach to restoring full arch length with maxillary fixed implant reconstruction: The PATZi protocol. The International Journal of Oral & Maxillofacial Implants, 38(5), 996-1004.
Holtzclaw, D. (2023). Remote anchorage solutions for severe maxillary atrophy: Zygomatic implants, pterygoid implants, transnasal implants, piriform rim implants, nasopalatine implants, and trans-sinus dental implants. Zygoma Partners, LLLP
(図1)
a) 44歳の女性患者.歯周病および外傷による骨喪失を認める.
b) 術前の患者の臨床状況
c) 本症例においては,PATZiアルゴリズムに従い,まず両側に翼状突起インプラント(P1)を配置した.次いで前部領域に注目した結果,両側の歯槽内インプラントでは初期固定が確保されなかったため,側鼻壁骨を固定する歯槽外インプラント(A2)を配置した.さらに,従来型の傾斜インプラントおよび経洞インプラントを試みたが,いずれも初期固定が達成されなかったため(Tx),PATZiプロトコルが示すザイゴマインプラントの適応に従い,Z1形態のザイゴマインプラントを配置し,満足のいく結果を得た.
d) 最終補綴物装着後の臨床写真,6か月後のハイブリッド補綴物によるリハビリテーションの臨床写真.
The Glossary of Prosthodontic Terms 2023: Tenth Edition. (2023). The Journal of prosthetic dentistry,
130(4 Suppl 1), e1–e3.
Bedrossian, E., Sullivan, R. M., Fortin, Y., Malo, P., & Indresano, T. (2008). Fixed-prosthetic implant restoration of the edentulous maxilla: a systematic pretreatment evaluation method. Journal of oral and maxillofacial surgery : official journal of the American Association of Oral and Maxillofacial Surgeons, 66(1), 112–122.
Zarb, George & Bolender, C.L.. (2004). Prosthodontic treatment for edentulous patients: complete dentures and implant-supported prostheses. 12 th ed. St. Louis: Mosby Inc. 190-207.
Schwarz F, Schär A, Nelson K, Fretwurst T, Flügge T., & Ramanauskaite A, Recommendations for Implant-Supported Full-Arch Rehabilitations in Edentulous Patients: The Oral Reconstruction Foundation Consensus Report. International Journal of Prosthodontics. 2021;34.
Maló, P., Rangert, B., & Nobre, M. (2003). "All-on-Four" immediate-function concept with Brånemark System implants for completely edentulous mandibles: a retrospective clinical study. Clinical implant dentistry and related research, 5 Suppl 1, 2–9.
Ponnusamy, S., Gonzalez, J., & Holtzclaw, D. (2023). A systematic approach to restoring full arch length with maxillary fixed implant reconstruction: The PATZi protocol. The International Journal of Oral & Maxillofacial Implants, 38(5), 996-1004.
Holtzclaw, D. (2023). Remote anchorage solutions for severe maxillary atrophy: Zygomatic implants, pterygoid implants, transnasal implants, piriform rim implants, nasopalatine implants, and trans-sinus dental implants. Zygoma Partners, LLLP
Soluciones de anclaje remoto para maxilares atróficos: Aplicación del protocolo PATZi en pacientes de la
Facultad de Odontología, UFM – Serie de casos
Jimmy Sandoval 1)Rodrigo Cayarga 1,3)Erick Lima 1,3)Luis Grisolía 2,3)Juan Gonzalez 3)
1) Advanced Implantology Department. Faculty of Dentistry, Francisco Marroquín University, Guatemala.
2) Restorative Department. Faculty of Dentistry, Francisco Marroquín University, Guatemala.
3) Continues Education Department. Faculty of Dentistry, Francisco Marroquín University, Guatemala.
Resumen
La atrofia ósea maxilar, caracterizada por una reducción de la densidad ósea y una disminución de la altura y el grosor, presenta desafíos significativos durante las fases quirúrgica y restauradora del tratamiento con implantes dentales. La rehabilitación tradicional con prótesis completas soportadas por la mucosa a menudo genera incomodidad en el paciente, estabilidad protésica limitada y reabsorción ósea alveolar progresiva. En contraste, las prótesis soportadas por implantes han surgido como una solución superior, proporcionando mejor retención, estabilidad y función masticatoria. Sin embargo, la deficiencia de volumen óseo y la distribución inadecuada en el sentido anteroposterior suelen dificultar la colocación de implantes en maxilares atróficos.
El protocolo PATZi ha sido desarrollado como un enfoque sistemático para abordar estos desafíos, utilizando tanto implantes dentales convencionales como implantes de anclaje remoto para optimizar la rehabilitación protésica en maxilares atróficos. Este protocolo permite la carga inmediata de prótesis fijas provisionales mediante un algoritmo estructurado que prioriza la colocación de los implantes en función de la idoneidad anatómica y la estabilidad primaria.
La secuencia comienza con los implantes pterigoideos (P1) y continúa con los sitios de anclaje bicortical anterior (A1 o A2), seguidos de implantes angulados convencionales en la región premolar (T1 o T2). Los implantes cigomáticos (Z1, Z2, Z3) se utilizan como último recurso en casos de estabilidad insuficiente.
Al establecer un marco quirúrgico claro, el protocolo PATZi garantiza resultados consistentes y facilita la carga protésica inmediata, con un torque de inserción recomendado de al menos 30 Ncm por implante o un total de 120 Ncm. Este enfoque innovador mejora la satisfacción del paciente, la función protésica y el éxito a largo plazo en la rehabilitación de maxilares atróficos.
La atrofia ósea maxilar se define como la reabsorción ósea que se percibe clínicamente por una disminución en la densidad ósea y una reducción en altura y grosor,1 lo que complica las fases quirúrgicas y restaurativas de los implantes dentales. La rehabilitación de estos pacientes, asegurando estabilidad protésica, fonética adecuada y una función masticatoria estable, representa un desafío importante.2
El tratamiento convencional para estos pacientes ha sido durante mucho tiempo la dentadura completa soportada por mucosa, un dispositivo acrílico destinado a reemplazar tejidos duros y blandos perdidos (como dientes y tejidos atróficos), siendo un dispositivo removible estrictamente soportado por la mucosa maxilar.1
Las desventajas de la dentadura completa incluyen la falta de estabilidad, soporte y retención de la prótesis en los tejidos, lo que se traduce en incomodidad para el paciente, ya que puede causar irritación en los tejidos blandos.3 Además, el uso de una dentadura completa soportada por mucosa puede resultar en una atrofia continua del hueso alveolar, tanto en sus dimensiones verticales como horizontales.2
La solución ideal es la prótesis soportada por implantes, ya que proporciona una alta calidad de vida y satisfacción a los pacientes, relacionada con la retención, estabilidad y facilidad de masticación.4 La configuración All-on-4, propuesta por P. Maló,5 ha sido ampliamente adoptada para la restauración de prótesis soportadas por implantes dentales. Sin embargo, un problema común en implantología es la falta de volumen óseo y la distribución anteroposterior deficiente.6
En este contexto, el protocolo PATZi ha surgido como una técnica prometedora para la rehabilitación protésica en maxilares atróficos. Este protocolo es un algoritmo sistemático que se centra en el uso de implantes dentales convencionales (angulados, paralelos) y de anclaje remoto (pterigoideos, nasopalatinos, espina nasal, transnasales, transinusales, cigomáticos) siguiendo una secuencia lógica. El objetivo principal es permitir la carga inmediata de una prótesis fija provisional.6
El protocolo PATZi describe una secuencia quirúrgica para la colocación de implantes dentales en maxilares atróficos utilizando un enfoque sistemático: comienza con la colocación de implantes pterigoideos (P1) en la región molar del maxilar. Si no se logra una estabilidad primaria adecuada, se clasifica como fallido (Px).6,7
El siguiente paso es la colocación de implantes dentales en la región anterior del maxilar con anclaje bicortical. Se utilizan áreas anatómicas como la espina nasal, el hueso piriforme y la pared lateral de la nariz (categoría A1). Si estas áreas están contraindicadas, se emplean implantes dentales transnasales (categoría A2). Si no se logra el torque de inserción requerido, se clasifica como fallido (Ax). Los implantes convencionales angulados se colocan en la región premolar sin anclaje bicortical (categoría T1). Si esto no es posible, se utiliza anclaje remoto en la pared lateral nasal (categoría T2). Si no se obtiene la estabilidad primaria requerida, se clasifica como fallido (Tx).6,7
Finalmente, si cualquiera de las categorías anteriores falla, se utilizan implantes dentales cigomáticos como último recurso. Estos pueden colocarse en la región premolar (Z1), molar (Z2) o anterior (Z3), dependiendo del sitio de emergencia del implante.6,7
El protocolo PATZi proporciona un marco consistente y sistemático para la colocación de implantes dentales en maxilares atróficos, garantizando una configuración biomecánica adecuada y facilitando la carga inmediata de prótesis soportadas por implantes dentales. Aunque no se ha establecido un torque de inserción mínimo específico, generalmente se requiere un mínimo de 30 Ncm por implante o un torque total de inserción de 120 Ncm para permitir la carga inmediata.6 Este protocolo ayuda a los cirujanos a lograr resultados consistentes y planificar intervenciones futuras necesarias.
El protocolo PATZi aplicado:
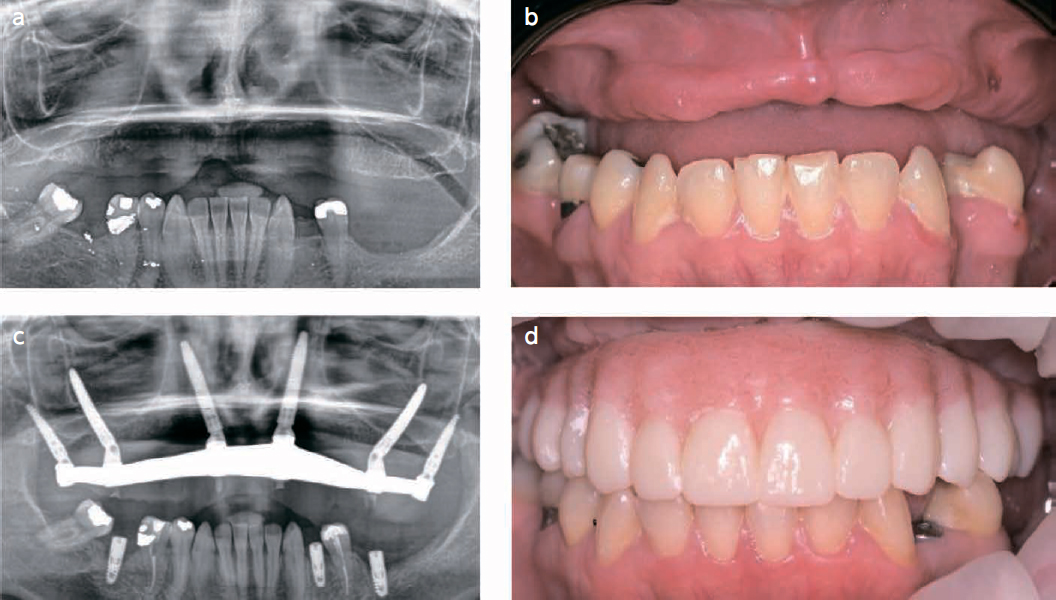
(Fig.1)
a) Paciente femenina de 44 años con pérdida ósea debido a enfermedad periodontal y una lesión traumática.
b) Situación clínica de la paciente antes de la cirugía.
c) Siguiendo el algoritmo PATZi en este caso, primero se colocaron implantes pterigoideos bilaterales (P1). Luego se dirigió la atención a la región anterior, donde los implantes intraalveolares bilaterales no lograron estabilidad primaria, por lo que se lograron implantes extraalveolares que comprometieron el hueso de la pared nasal lateral (A2). Se intentaron implantes tradicionales inclinados e implantes transinusales, pero no mostraron estabilidad primaria (Tx). El protocolo PATZi demostró la indicación de implantes cigomáticos, por lo que se colocaron satisfactoriamente implantes cigomáticos en configuración Z1.
d) Fotografía clínica después de la entrega de la prótesis final, rehabilitación con prótesis híbrida después de 6 meses.
Objetivo:
El objetivo de esta serie de casos es contribuir a la documentación presentando la aplicación del protocolo PATZi en maxilares atróficos.
Materiales y métodos:
Quince pacientes con maxilares atróficos se presentaron en la clínica dental de la Facultad de Odontología de la Universidad Francisco Marroquín entre enero de 2023 y octubre de 2023. Los pacientes fueron tratados quirúrgicamente utilizando el protocolo PATZi por el personal de cirujanos de O.R.C.A.A.
Se colocó un total de 112 implantes dentales, incluidos 30 implantes pterigoideos (P), 30 implantes anteriores (A) y 30 implantes inclinados (T). Debido a la falta de estabilidad primaria (≥35N) para lograr la carga inmediata de la prótesis y mejorar la distribución anteroposterior, se colocaron 22 implantes
cigomáticos (Zi).
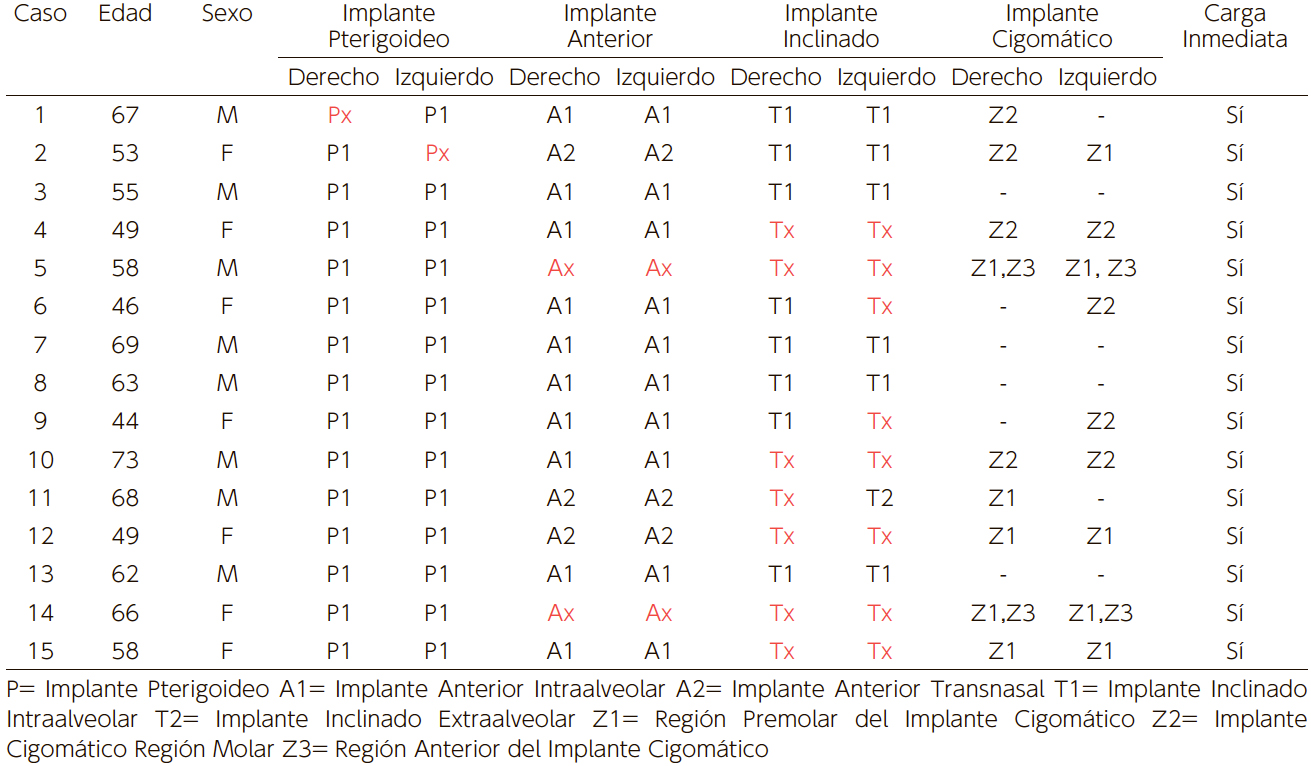
Por lo tanto, se colocaron 10 implantes cigomaticos con la plataforma emergiendo en la región premolar (Z1), 8 implantes en la región molar (Z2) y 4 implantes en la región anterior (Z3). Se recopilaron datos demográficos preoperatorios y, para comprender la aplicación del protocolo PATZi, se midieron la estabilidad primaria de los implantes inmediatos y la posibilidad de carga inmediata después de la cirugía de la prótesis (Tabla 1).
(Tabla 1) Demografía, estabilidad primaria del implante y carga inmediata de la prótesis.
Resultados:
De los 15 pacientes tratados con el protocolo PATZi, 7 fueron mujeres y 8 fueron hombres, con un rango de edad de 44 a 73 años. De los 112 implantes colocados, 28/30 implantes pterigoideos, 26/30 implantes anteriores (20 intraalveolares (A1), 6 transnasales (A2)) y 15/30 implantes inclinados mostraron estabilidad primaria. Todos los pacientes recibieron carga inmediata de los implantes dentales después de la cirugía.
Conclusiones e implicaciones clínicas:
El protocolo PATZi, en manos de clínicos expertos, que incorpora tanto implantes convencionales como de anclaje remoto, resuelve casos de atrofia maxilar severa y es una alternativa viable para lograr estabilidad primaria y obtener carga inmediata de implantes dentales. En casos particulares donde no se logró estabilidad primaria para carga inmediata ni una distribución anteroposterior adecuada, se indica la colocación de implantes cigomáticos.
Sin embargo, el período de observación en este estudio puede ser demasiado corto para evaluar completamente el éxito o fracaso a largo plazo del protocolo. Las observaciones de seguimiento deben incluir la evaluación de la longevidad de los implantes, la estabilidad protésica y el monitoreo de posibles complicaciones como fallos de implantes, reabsorción ósea o desajuste de prótesis. Las evaluaciones posquirúrgicas regulares, incluyendo análisis radiográficos y exámenes clínicos a los 6 meses, 1 año y anualmente después de eso, proporcionarían una comprensión más completa de la eficacia y seguridad a largo plazo del protocolo. Se necesitan estudios futuros con períodos de seguimiento más prolongados para validar estos hallazgos y refinar aún más la aplicación del protocolo PATZi
References
The Glossary of Prosthodontic Terms 2023: Tenth Edition. (2023). The Journal of prosthetic dentistry,
130(4 Suppl 1), e1–e3.
Bedrossian, E., Sullivan, R. M., Fortin, Y., Malo, P., & Indresano, T. (2008). Fixed-prosthetic implant restoration of the edentulous maxilla: a systematic pretreatment evaluation method. Journal of oral and maxillofacial surgery : official journal of the American Association of Oral and Maxillofacial Surgeons, 66(1), 112–122.
Zarb, George & Bolender, C.L.. (2004). Prosthodontic treatment for edentulous patients: complete dentures and implant-supported prostheses. 12 th ed. St. Louis: Mosby Inc. 190-207.
Schwarz F, Schär A, Nelson K, Fretwurst T, Flügge T., & Ramanauskaite A, Recommendations for Implant-Supported Full-Arch Rehabilitations in Edentulous Patients: The Oral Reconstruction Foundation Consensus Report. International Journal of Prosthodontics. 2021;34.
Maló, P., Rangert, B., & Nobre, M. (2003). "All-on-Four" immediate-function concept with Brånemark System implants for completely edentulous mandibles: a retrospective clinical study. Clinical implant dentistry and related research, 5 Suppl 1, 2–9.
Ponnusamy, S., Gonzalez, J., & Holtzclaw, D. (2023). A systematic approach to restoring full arch length with maxillary fixed implant reconstruction: The PATZi protocol. The International Journal of Oral & Maxillofacial Implants, 38(5), 996-1004.
Holtzclaw, D. (2023). Remote anchorage solutions for severe maxillary atrophy: Zygomatic implants, pterygoid implants, transnasal implants, piriform rim implants, nasopalatine implants, and trans-sinus dental implants. Zygoma Partners, LLLP